
In the tightrope procedure, the knee is stabilized with a soft but very strong (250 pounds of tensile strength) suture called fiber tape that runs along the lateral side of the knee joint. This procedure is best illustrated in the picture below:
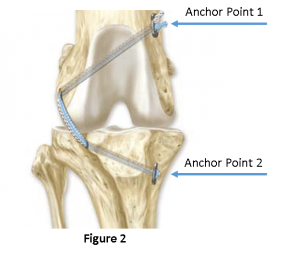
The fixation points that anchor the suture make this procedure unique among other suture techniques in that they utilize the hard outer cortex of the long bones as fixation points. This creates a very effective manner in which to anchor the suture, and does so in a way that maximizes stabilization of the joint while maximizing comfort and range of motion.
In TPLO, The philosophy behind the surgery is to change the angle of the Tibial Plateau, which is the area where the Femur and the Tibia interact and communicate. By doing so, this eliminates the need for the CCL ligament entirely and returns stability to the joint itself by flattening the head of the tibia and eliminating shear forces across the plateau (the main function of the CCL ligament is to counter shear forces that inevitably pull the tibia forward when walking and running). In order to accomplish this, a portion of the head of the tibia is cut, rotated, and plated in place. The diagram below shows how this works.

In TTA, unlike TPLO. the angle of the tibial plateau is not directly reduced but instead is functionally reduced in a somewhat different manner. Instead of cutting and rotating the entire tibial head, a smaller portion of front part of the bone called the tibial tuberosity is cut and extended forward. A relevant analogy as to how this works would be to consider a steep ramp. By extending the length of the ramp, one can effectively decrease the steepness of the angle of the ramp. More importantly, TTA also creates tension on the large and strong patellar tendon that runs over the patella and inserts the quadriceps muscle group into the proximal tibia. The subsequent tension removes forward instability caused by the ruptured CCL providing stabilization on two fronts.

The MMP is really little more than a modification of the TTA in that it has the same net effect as the TTA, only rather than using a cage and spacer to extend the tibia, a titanium wedge called Orthofoam is used. The main difference between traditional TTA and the MMP is that the MMP does not require any screws to keep it in place. The titanium Orthofoam wedge that is placed consists of a very strong but semi-porous matrix that grips the surrounding bone and facilitates bone formation around and within its structure. The gripping effect enables only the placement of a small pin and staple to keep it in place, significantly reducing surgical time and invasiveness; leading to quicker weight bearing and healing (4-6 weeks versus 8-12 weeks with other procedures): With a lesser burden of hardware implanted in comparison to TTA, there is less tendency for complication and/or reaction to the hardware. The titanium material used is also less reactive to biological systems and is more resistant to bacterial growth and subsequent infection than other metal implantation materials.

My preference for CCL surgical repair in dogs 40 pounds or larger is MMP, but still prefer tightrope for dogs under 40 pounds. Other factors that determine the best procedure for a given dog with a CCL tear depending are age, size, lifestyle, and unique anatomic characteristics of each individual patient.